Y’all. I have to tell you what happened.
Last summer, at 41 years old, I developed new-onset eczema.
On my EYELID. And under my eye. Of all the places on my body, it picked my face. Then, a few weeks later, a patch showed up on my neck like the party needed more guests.
I was furious. I was confused. I was LITERALLY doing everything right.
I was already using my Prequel skincare, which is formulated specifically for eczema- and rosacea-prone skin. When the flare wouldn’t quit, I stripped my routine down to the absolute bare bones. Topical hydrocortisone. Aquaphor. The most basic, boring, dermatologist-approved protocol you can do at home.
It would start to clear up… and then come right back. Over and over. For months.
Why would eczema suddenly show up in your 40s when you’ve never had it?
Turns out this is a real thing. And it’s way more common than anyone talks about.
Perimenopause does a number on your skin in ways most of us are never warned about. As estrogen starts to decline, your skin produces less oil, loses ceramides (the lipids that hold your skin barrier together), and the whole barrier function is compromised. Your skin microbiome shifts. Your immune response shifts. And the inflammation that your body used to handle quietly? Now it’s showing up on your face.
Research published in dermatology literature confirms that the drop in estrogen during perimenopause can trigger new-onset eczema or worsen existing eczema, even in women with no prior history. Skin gets thinner, drier, more reactive, and more easily inflamed.
So… cool. One more thing nobody tells you about your 40s.
But wait. Aren’t you on a GLP-1? Shouldn’t that be handling the inflammation?
This was literally my exact question. I’ve been on a GLP-1 for over two years. GLP-1s are known to reduce inflammation, even at low doses. So why was my face actively revolting?
GLP-1s reduce one type of inflammation, the metabolic kind. The kind driven by insulin resistance, visceral fat, and blood sugar dysfunction. And they do that really well.
But the inflammation driving perimenopausal skin changes is a different beast entirely. It’s hormonal. It’s local. It’s happening in my skin because my estrogen is dropping, my skin barrier is compromised, and my skin’s immune response is reacting to things it never used to.
GLP-1 is putting out the metabolic fire in my body. But the hormonal fire showing up in my skin needed something else.
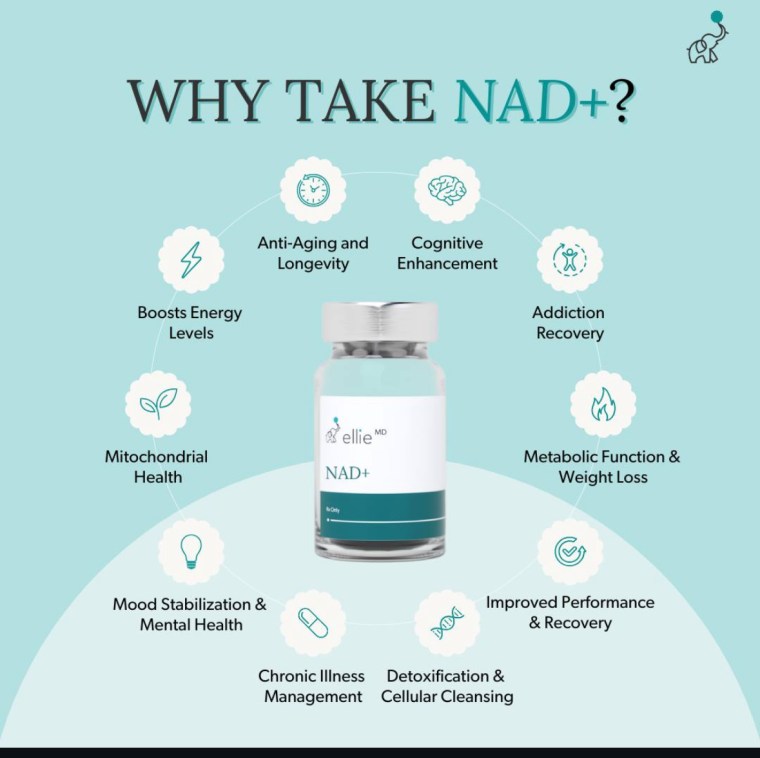
Enter NAD+

I started NAD+ injections last fall. I wasn’t taking them for my skin, honestly. I was taking them for energy, recovery, and general cellular function. You know, the perimenopausal brain fog. The skin improvement was surprising, but then when I thought about it, it made PERFECT SENSE.
But within a few weeks, I noticed my eczema was staying cleared up. Not in the “it’s better today, let’s see what happens tomorrow” way. In the actually gone way.
I added GHK-Cu later, which also has some skin benefits, but I want to be really clear. The eczema had already cleared before I added GHK-Cu. The NAD+ was doing the heavy lifting.

And then I did what nurses do, which is make absolutely terrible patients. I got busy. I skipped a week. Then another one.
Guess what came back.
I went straight to my kitchen, pulled my vial out of the fridge, and took my injection. It cleared up again after a couple of weeks. Then I missed another week (I KNOW, I KNOW). Started seeing the early signs creeping back. Back to the kitchen I went. I also bumped up to tier 2 dosing, which is a higher dose, and the skin kept improving. Not getting worse. Which matters to me because it tells me my skin is responding to more NAD+, not less.
At this point, I am not messing around. NAD+ is in my toolbelt permanently.
But is there actual science behind this, or am I just seeing things?
I want to be honest with you here, because I am not trying to oversell anything.
Research on NAD+ and inflammatory skin conditions is still in its early stages. But what’s out there looks really promising.
NAD+ is a molecule every cell in your body uses to make energy and repair itself. When you’re young, you have a lot of it. As you age, levels drop. When NAD+ drops, your cells can’t handle stress as well, can’t repair damage as well, and can’t calm inflammation as well.
One 2023 study found that boosting NAD+ calmed down one of the main inflammation pathways (called Th17) that drives skin conditions like eczema and psoriasis. Basically, more NAD+ told the inflammation to settle down.
Another study on a form of NAD+ showed it reduced eczema symptoms, itching, and helped the skin barrier rebuild itself. It calmed the fire AND helped the wall.
And a big review from 2025 on a related form of vitamin B3 (nicotinamide) laid out why this whole family of molecules is already being used by dermatologists for eczema, rosacea, and other inflammatory skin issues.
So no. This is not me seeing things.
It’s me having a body that was inflamed, a skin barrier that was compromised, a hormonal transition nobody warned me was starting, and a cellular molecule (NAD+) that supports the exact repair and anti-inflammation work my skin needed.
It makes sense that it worked. It makes sense that when I stopped, it came back. And it makes sense that when I bumped up my dose, it kept improving.

What I want you to hear:
If you’re in your late 30s or 40s and something new is showing up on your skin, whether that’s eczema, rosacea flares, random dryness, or sensitivity you never had before, this is worth paying attention to. Your skin is telling you your hormones are shifting. That’s just physiology.
And if you’re already in the longevity and anti-aging conversation and you’re curious about NAD+ for energy, recovery, collagen, mitochondrial health… all the things… this is one more reason to pay attention. The skin benefits are real, even if the research is still catching up.
NAD+ is not a miracle cure. The research is preliminary. Anyone who tells you otherwise is selling you something.
But for me? It’s part of the stack now. PERMENANTLY
If you’re curious about NAD+ or want to actually talk to a provider about whether it’s something worth exploring for you, I use EllieMD for my telehealth. The physicians are real, the messaging is unlimited, and you can ask all the questions you need to ask before you start anything. (They work with CloveRX for compounding, which is the pharmacy that actually makes the peptides. Same consistent quality every single time, which is what I wanted when I made the switch.) With EllieMD you now have the option of NAD+ Injections or an NAD+ Nasal Spray (which I will probably try out with my next order).
As always, talk to your own provider, do your own research, and don’t start anything without understanding what it does and what it doesn’t do. I am a nurse, but I am not YOUR nurse, and this is not medical advice. It’s my story, the research I’ve pulled, and an invitation to look into it if it resonates.
Love you, mean it.
XOXO,
NIKI, RN
PCOS. Perimenopause. Metabolic health. The real stuff. Not just “eat less, move more.”
ASK ME ANYTHING
TRUSTED WELLNESS TOOLS
Not sure where to start? Take my free quiz and I’ll send you a custom plan.
WHAT’S RIGHT FOR MY BODY?
P.S. Missed the previous editions of The Nurse’s RX?
↓ Catch up here ↓
READ PAST EDITIONS
↓ LET’S CONNECT ↓




Let’s be clear about who I am (and who I’m not)
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing here replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
Scope of practice
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment. These statements have not been evaluated by the FDA. Products discussed are not intended to diagnose, treat, cure, or prevent any disease.
Transparency
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links in this email are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate, I earn from qualifying purchases.
Results + Testimonials
Any testimonials or results shared here reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
Read the full fine print at nicoleinscrubs.com/disclosure
No longer wish to receive these emails? UNSUBSCRIBE HERE