Can I tell you the thing that still makes me want to flip a table?
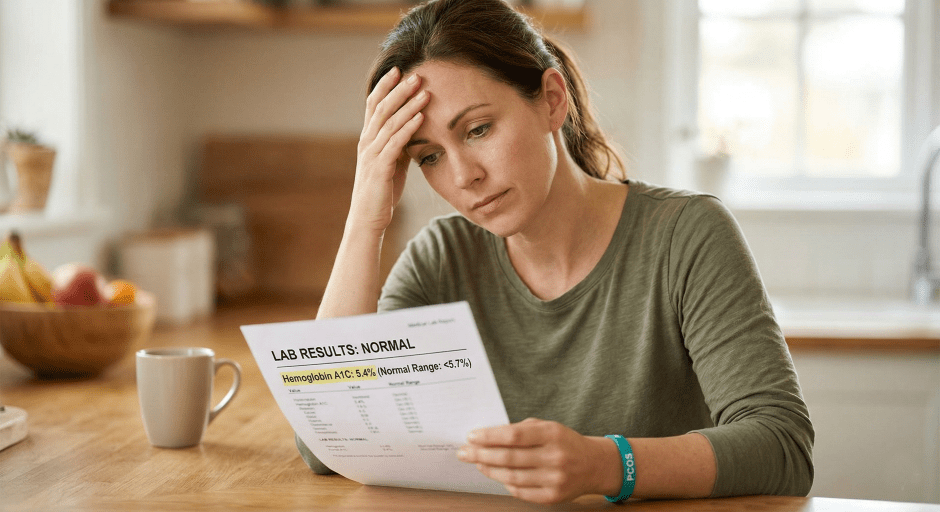
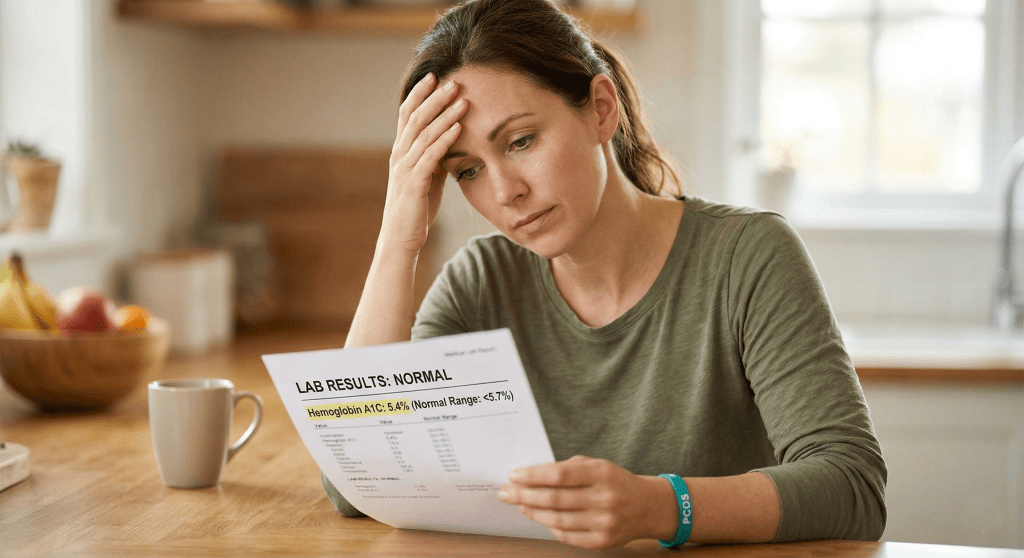
It’s the phrase “your labs are normal.”
Because for a lot of women… especially women with PCOS, perimenopause knocking, and years of “borderline” results that nobody ever actually addressed… “normal” doesn’t mean fine. It means nobody looked deep enough.
Here’s what most routine bloodwork checks when it comes to blood sugar: fasting glucose and A1C. That’s it.
And here’s what those tests miss: how hard your body is working to keep those numbers where they are.
Your fasting glucose could be sitting at a perfect 94 mg/dL. Your A1C could be a beautiful 5.4%. And your pancreas could be GRINDING out insulin behind the scenes just to hold those numbers in place. You wouldn’t know. Because nobody ordered the test that shows it.
That test is called fasting insulin. And when you pair it with your fasting glucose, you can calculate something called your HOMA-IR score… which basically tells you how insulin resistant your body is right now.
Not how your blood sugar looks on paper. How your body is actually functioning.
The CDC says over 115 million American adults have prediabetes. 8 in 10 don’t know it. That’s not because they’re ignoring their health. It’s because the standard tests aren’t catching it early enough.
And research published in Diabetes Care found that using A1C alone to screen for prediabetes missed about 75% of at-risk people.
If that doesn’t make you want to flip the table too… I don’t know what will.
Here’s what I want you to do:
Next time you have bloodwork, ask your doctor to add a fasting insulin level. It’s drawn from the same blood, at the same time. You may need to specifically request it because it’s not included in standard panels.
Once you have it, here’s the math: (fasting glucose x fasting insulin) / 405 = your HOMA-IR score. Under 1.0 = optimal. Over 2.5 = insulin resistance may be present. Over 3.0 = significant.
That one number could explain more about why you feel the way you feel than every “normal” result you’ve ever gotten combined.
I wrote a full deep dive on this on the blog… why standard panels miss it, what it means if you have PCOS, and the exact labs I’d tell my best friend to ask for. If you want the whole picture, it’s there for you.
Not sure where to start? Take my free quiz and I’ll send you a custom plan.
WHAT’S RIGHT FOR MY BODY?
P.S. Missed the previous editions of The Nurse’s RX? ↓ Catch up here ↓
READ PAST EDITIONS
↓ LET’S CONNECT ↓
Let’s be clear about who I am (and who I’m not)
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing here replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
Scope of practice
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment. These statements have not been evaluated by the FDA. Products discussed are not intended to diagnose, treat, cure, or prevent any disease.
Transparency
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links in this email are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate, I earn from qualifying purchases.
Results + Testimonials
Any testimonials or results shared here reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
You leave your doctor’s appointment with the same answer you’ve gotten for the last five years. “Everything looks good. Labs are normal.”
And you sit in your car and think… then why do I feel like this? Why am I exhausted by 2pm every day? Why can’t I lose weight no matter what I do? Why does my brain feel like it’s running through fog? Why am I doing everything “right” and nothing is changing?
You’ve heard “your labs are normal” so many times that you’ve started to believe the problem must be you. Your discipline. Your effort. Your willpower.
It’s not you. And I need you to hear that.
Your labs might technically be within range. But “within range” and “optimal” are not the same thing. And the test that would actually tell you whether you have insulin resistance? There’s a very good chance your doctor never ordered it.
What Is a Fasting Insulin Test and Why Don’t Most Doctors Order It?
When you go in for your annual physical or routine bloodwork, your doctor typically checks two things related to blood sugar: your fasting glucose and your A1C (hemoglobin A1C).
Fasting glucose is a snapshot. It tells you what your blood sugar is right now, after you haven’t eaten for 8 to 12 hours. A result under 100 mg/dL is considered normal. Between 100 and 125 is prediabetes. Over 126 is diabetes.
A1C is a wider view. It measures your average blood sugar over the last 2 to 3 months by looking at how much sugar has attached to your red blood cells. Under 5.7% is normal. 5.7 to 6.4% is prediabetes. Over 6.5% is diabetes.
Both of these tests measure the same thing… glucose. They just measure it differently.
And here’s the problem: neither one tells you how hard your body is working to keep that glucose number “normal.”
Think of it this way. Imagine two women sitting in the same doctor’s office on the same day. Both have a fasting glucose of 94 mg/dL. Both A1Cs come back at 5.4%. Both get told their labs are normal.
But behind the scenes, the first woman’s pancreas is producing 5 units of insulin to maintain that glucose level. Easy. No sweat. Her metabolic system is cruising.
The second woman’s pancreas is grinding out 18 units of insulin just to hold the line at 94. Her body is working triple shifts to keep that number where it is. She’s exhausted, gaining weight she can’t explain, brain fog is constant, and she can’t stop thinking about food.
On paper, they look identical. Metabolically, they’re in completely different places.
The only way to see the difference? A fasting insulin test. And most routine bloodwork panels do not include it.
That’s not an oversight by your specific doctor. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) states plainly that doctors use blood tests to find out if someone has prediabetes, but they don’t usually test for insulin resistance. It’s just not part of the standard protocol. Which means millions of women are walking around with insulin resistance that nobody is looking for… because nobody is ordering the test that would find it.
What Is HOMA-IR and How Do You Calculate It?
A fasting insulin test measures how much insulin your pancreas is producing after you haven’t eaten. That number alone is helpful. But when you combine it with your fasting glucose, you can calculate something even more useful… your HOMA-IR score (Homeostatic Model Assessment of Insulin Resistance). This is essentially a number that tells you how insulin-resistant your body is.
The math is simple: (fasting glucose x fasting insulin) / 405.
Both values must come from the same fasting blood draw.
Here’s how to read your HOMA-IR score: Under 1.0 — Optimal insulin sensitivity. Your body is using insulin efficiently. 1.0 to 2.5 — Moderate range. Worth watching, especially if you have other risk factors like PCOS, family history of diabetes, or unexplained weight gain. Over 2.5 — Insulin resistance is likely present. Your pancreas is working harder than it should to keep your blood sugar in range. Over 3.0 — Significant insulin resistance. This level may already be driving symptoms… fatigue, weight gain, brain fog, food noise… even if your glucose and A1C still look completely normal on paper.
So why doesn’t your HOMA-IR show up on your standard bloodwork? A few reasons. Most standard metabolic panels are built around glucose, not insulin. Time constraints in a 15-minute appointment don’t leave room for expanded testing. And many providers follow a “wait and see” approach to borderline results… meaning they don’t dig deeper until your numbers actually cross into prediabetes or diabetes territory.
By then, the damage has been building for years.
Can You Have Insulin Resistance with Normal Blood Sugar and a Normal A1C?
Yes. And this is the part that makes me want to flip a table.
Your fasting glucose can be perfect. Your A1C can be textbook. And insulin resistance can still be building behind the scenes for years because your pancreas is compensating… producing more and more insulin to keep your blood sugar in range.
According to the Cleveland Clinic, as long as your pancreas can make enough insulin to overcome the resistance, your blood sugar levels will stay in a healthy range and you won’t have any symptoms. But over time, the cells that make insulin can wear out. That’s when blood sugar finally rises. That’s when you get the prediabetes or diabetes diagnosis. But the insulin resistance? That started long before the numbers changed.
Research from a peer-reviewed study published in a PMC journal found that elevated insulin levels in the absence of impaired glucose tolerance and normal A1C may actually be a much earlier indicator of metabolic disease risk than glucose or A1C alone. In other words… insulin was waving a red flag the whole time. Nobody was watching for it.
How Many People Have Undiagnosed Insulin Resistance and Prediabetes?
According to the CDC’s most recent National Diabetes Statistics Report (January 2026), over 115 million American adults have prediabetes. And 8 in 10 of them don’t know it.
Let that sink in for a second. 80% of people with prediabetes are walking around right now being told their labs are normal.
On top of that, research published in Diabetes Care found that using A1C alone to screen for prediabetes missed about 75% of at-risk individuals. The study specifically noted that A1C was less sensitive for detecting at-risk individuals compared to fasting glucose and glucose tolerance testing… and none of those tests even measure insulin.
Meanwhile, a growing body of research shows that elevated insulin levels can appear years… and according to some researchers, potentially even decades… before blood sugar ever crosses into an abnormal range. Your pancreas is working overtime to keep your glucose normal, and nobody’s checking to see how hard it’s working.
Why Insulin Resistance Testing Matters Even More If You Have PCOS
If you have polycystic ovary syndrome, this isn’t just relevant. It may be the entire missing piece of your health puzzle.
Research estimates that insulin resistance affects between 50 and 80% of women with PCOS… including women who are not overweight. That’s not a small subset. That’s the majority. And many of those women have never had their insulin levels checked.
Insulin resistance in PCOS doesn’t just affect blood sugar. It directly drives excess androgen (testosterone) production, which can cause irregular periods, acne, hair loss, excess body hair, and difficulty getting pregnant. The cycle looks like this: insulin resistance leads to higher insulin levels, which triggers increased androgen production, which disrupts ovulation, which worsens PCOS symptoms. It feeds itself.
And the whole time, your fasting glucose and A1C may look completely normal because your pancreas is compensating.
One peer-reviewed study in the Journal of Clinical Medicine proposed that the medical community needs to shift from a “glucose-centric” approach to an “insulin-centric” model when managing PCOS… because by the time glucose rises, the metabolic damage has already been happening for years. The study emphasized that early identification of insulin resistance would enable timely intervention and could reduce the risk of long-term metabolic and reproductive complications.
If you’ve been told your labs look fine but you’re still gaining weight, still exhausted, still struggling with PCOS symptoms that nobody can explain… this may be why. The right labs were never ordered.
What Blood Tests Should You Ask Your Doctor For?
Ask for a fasting insulin test at your next appointment.
It’s a simple blood draw done at the same time as your regular fasting labs.
You may need to specifically request it… many providers won’t think to order it unless you ask.
If your provider pushes back, you can explain that you’d like to assess insulin resistance beyond what glucose and A1C alone can show.
The NIDDK confirms that providers don’t usually test for insulin resistance as part of standard screening.
That doesn’t mean the test isn’t available or valuable. It means you may need to advocate for yourself.
Know your HOMA-IR score.
Once you have your fasting insulin and fasting glucose from the same blood draw, you can calculate it yourself:
(fasting glucose x fasting insulin) / 405.
Under 1.0 is optimal.
Over 2.5 starts to suggest insulin resistance.
Over 3.0 is significant.
There are also free HOMA-IR calculators online if math isn’t your thing.
Ask about a full hormone panel if you have PCOS or suspect it.
Fasting insulin
HOMA-IR
testosterone (total and free)
DHEA-S
LH
FSH
lipid panel
These give a much more complete picture of what’s happening metabolically and hormonally than glucose and A1C alone.
Know the difference between “normal range” and “optimal.”
Lab reference ranges are based on population averages… they tell you where most people fall, not where you should be for your best health.
A fasting glucose of 98 is technically “normal” but it’s not optimal.
An A1C of 5.6 is technically “normal” but it’s one decimal point from a prediabetes diagnosis.
Don’t let “in range” make you stop asking questions.
Trust your body.
If you feel like something is off, something probably is.
I was the woman in the car. I had PCOS. I had high blood pressure, high cholesterol, and sleep apnea. I was labeled pre-diabetic for about eight months in 2006… and then my A1C came back down and everybody moved on. Normal. Case closed.
Except my white blood cell count kept showing chronic inflammation. Nobody connected those dots. Nobody said “hey, your A1C looks better but let’s dig deeper into WHY your body is still inflamed, WHY you can’t lose weight, WHY none of this is adding up.”
I never got the right tests. I still haven’t. What I got was a doctor who finally looked at me and said… something isn’t adding up. The calories in versus calories out math wasn’t mathing. My body wasn’t responding the way it should have been. And instead of handing me another pamphlet, he prescribed a GLP-1.
That changed everything. But I think about how many years I spent blaming myself for something that had a physiological explanation nobody bothered to look for. How many times I white-knuckled a diet and watched the scale not move and thought it was ME.
I’m a NICU nurse. I believe in evidence. I believe in labs. But I also believe that the wrong labs… or the incomplete ones… can leave you blaming yourself for something that was never your fault.
If your doctor says your labs are normal but your body is screaming that something is wrong… believe your body. Then go get the right labs. The ones I’m telling you about in this post? I wish someone had told me about them ten years ago.
Frequently Asked Questions About Insulin Resistance and Lab Testing
Can you have insulin resistance with a normal A1C?
Yes. Insulin resistance can develop years before your A1C ever moves out of the normal range. Your pancreas compensates by producing more insulin to keep blood sugar stable. As long as it can keep up, your glucose and A1C may look fine on paper while insulin resistance builds underneath. A fasting insulin test or HOMA-IR calculation can reveal what glucose-based tests miss.
What is HOMA-IR and how do I get tested?
HOMA-IR stands for Homeostatic Model Assessment of Insulin Resistance. It’s not a separate blood test… it’s a calculation using two values from a single fasting blood draw: your fasting glucose and your fasting insulin. The formula is (fasting glucose x fasting insulin) / 405. A score under 1.0 is considered optimal. Over 2.5 suggests insulin resistance. Over 3.0 is significant. You’ll need to ask your doctor to order a fasting insulin level since it’s not included in standard metabolic panels.
Does a normal fasting glucose mean I don’t have insulin resistance?
Not necessarily. Your fasting glucose measures what your blood sugar is at one moment in time. It doesn’t tell you how much insulin your body needed to get it there. Two people can have the exact same fasting glucose but very different insulin levels… and very different levels of metabolic stress happening behind the scenes.
Why doesn’t my doctor test for insulin resistance?
Most standard bloodwork panels focus on glucose, not insulin. The NIDDK notes that providers don’t usually test for insulin resistance as part of routine screening. It’s not that the test doesn’t exist or isn’t valuable. It’s that the current standard of care doesn’t include it unless you specifically ask or your provider is thinking beyond the basics.
What blood tests should I ask for if I have PCOS?
For a more complete metabolic and hormonal picture, consider asking about: fasting insulin, fasting glucose (to calculate HOMA-IR), A1C, testosterone (total and free), DHEA-S, LH, FSH, and a full lipid panel. These tests together can reveal insulin resistance, hormonal imbalances, and metabolic risk factors that glucose and A1C alone would miss.
Is it too late to test for insulin resistance in my 40s?
No. Research shows that lifestyle and medical interventions can reduce the risk of progressing from insulin resistance to type 2 diabetes significantly… even in midlife. The earlier you identify insulin resistance, the more options you have. But “earlier” doesn’t mean it has to be your 20s. It means earlier than waiting for a diabetes diagnosis.
Not sure where to start? My free Wellness Strategy Quiz can help you figure out what to focus on first based on where you are right now
Lorenzo C, et al. “A1C Between 5.7 and 6.4% as a Marker for Identifying Pre-Diabetes, Insulin Sensitivity and Secretion, and Cardiovascular Risk Factors.” Diabetes Care. 2010;33(9):2104-2109.
Parker J. “Recognizing the Role of Insulin Resistance in Polycystic Ovary Syndrome: A Paradigm Shift from a Glucose-Centric Approach to an Insulin-Centric Model.” Journal of Clinical Medicine. 2025;14(12):4021.
“Hyperinsulinemia: An Early Biomarker of Metabolic Dysfunction.” PMC. 2023. pmc.ncbi.nlm.nih.gov/articles/PMC10186728
Cleveland Clinic — Insulin Resistance: What It Is, Causes, Symptoms & Treatment — my.clevelandclinic.org/health/diseases/22206-insulin-resistance
“Markers of Insulin Resistance in Polycystic Ovary Syndrome Women: An Update.” World Journal of Diabetes. 2022. pmc.ncbi.nlm.nih.gov/articles/PMC8984569
“Insulin Resistance, Metabolic Syndrome and Polycystic Ovaries: An Intriguing Conundrum.” Frontiers in Endocrinology. 2025.
Ezeh U, et al. “Detecting Insulin Resistance in Polycystic Ovary Syndrome: Purposes and Pitfalls.” PubMed. 2004.
This site contains affiliate links and/or brand partnership content. I may earn a commission at no extra cost to you.
LET’S BE CLEAR ABOUT WHO I AM (AND WHO I’M NOT).
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing on this site replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
SCOPE OF PRACTICE.
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment — this is not something that should be DIY’d. These statements have not been evaluated by the FDA. Products discussed on this site are not intended to diagnose, treat, cure, or prevent any disease.
TRANSPARENCY.
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links on this site are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate I earn from qualifying purchases.
RESULTS + TESTIMONIALS.
Any testimonials or results shared on this site reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
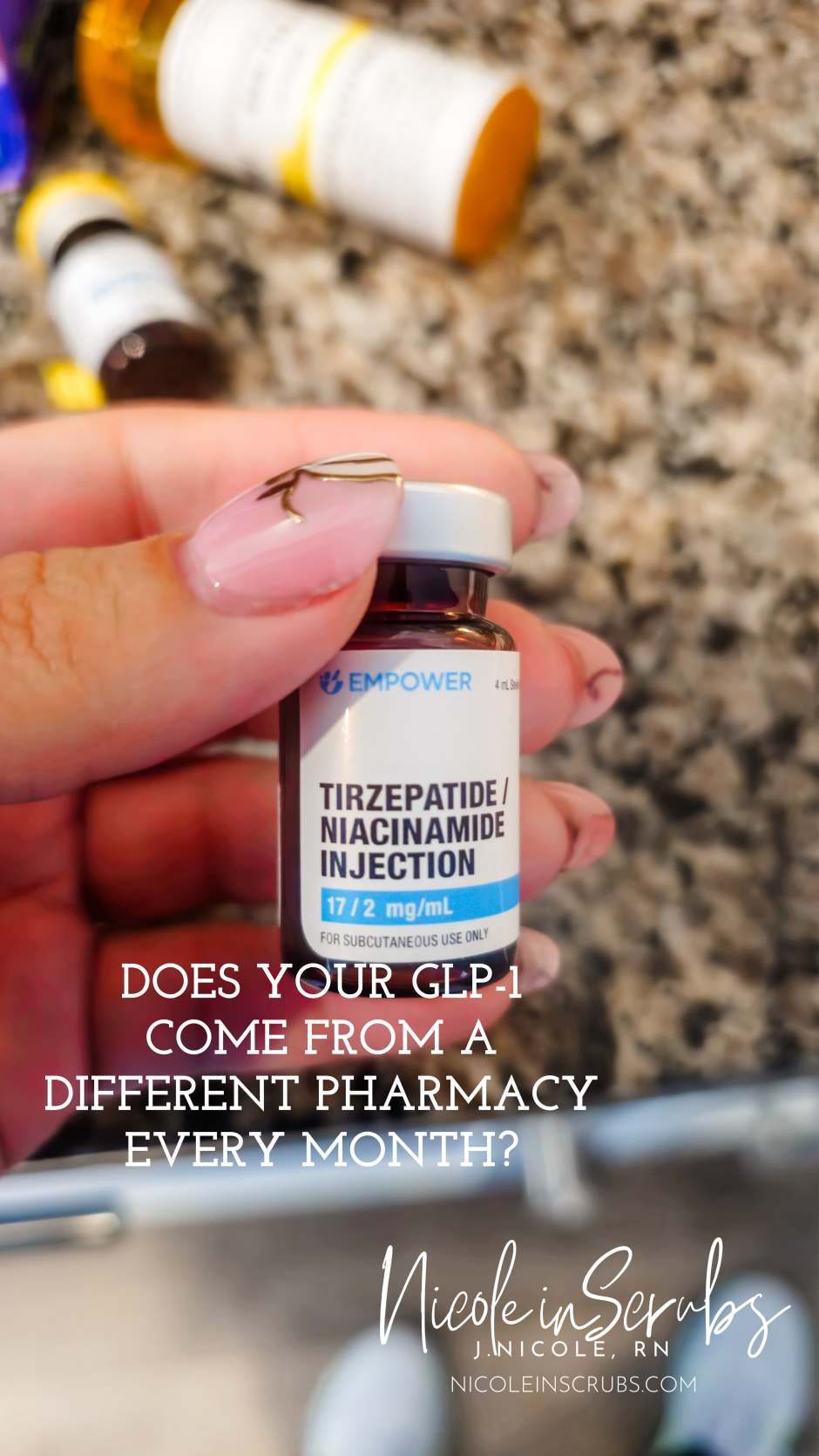
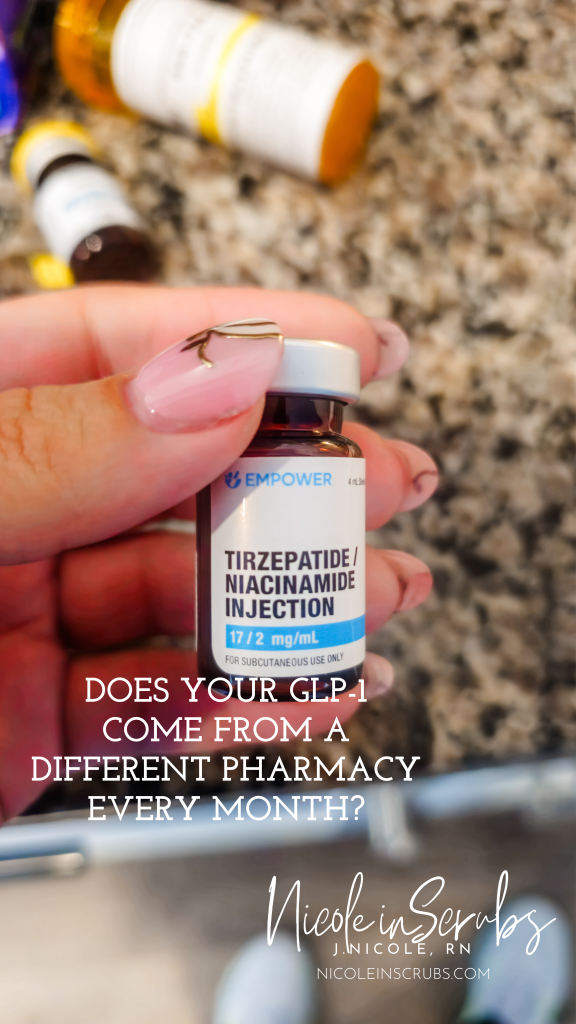
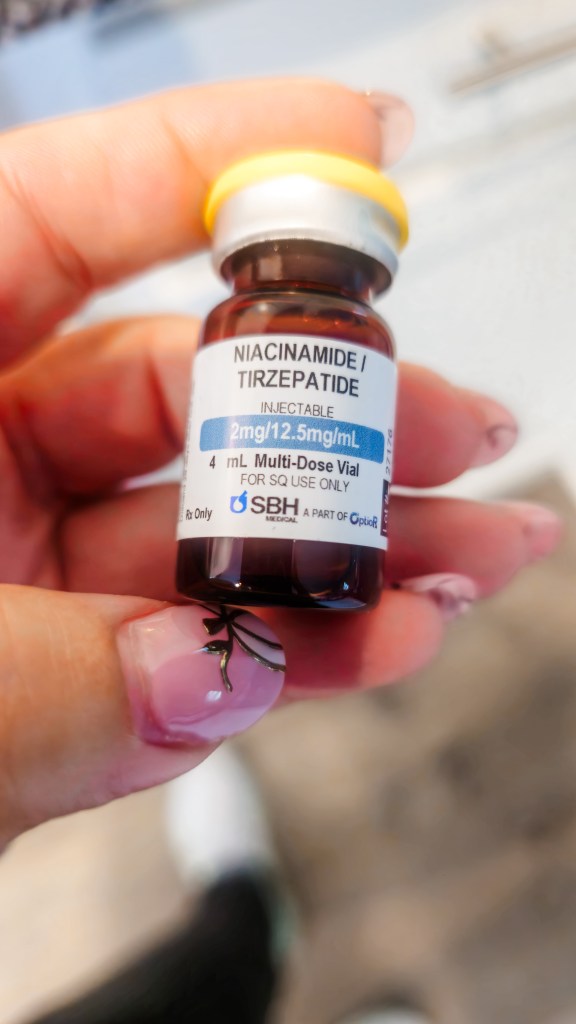
If you’re on a compounded GLP-1 medication through a telehealth company, there’s something you need to know… and most people have no idea it’s even happening.
It’s called pharmacy hopping. And it could be putting you at risk.
What Is GLP-1 Pharmacy Hopping?
Pharmacy hopping is when your telehealth company sends your prescription to a different compounding pharmacy each month. Not because anything is wrong with your prescription. Not because your dose changed. Just because of whatever deal or arrangement they have going on that month.
Here’s why that’s a problem. Every compounding pharmacy concentrates their GLP-1 medications differently. So even if your prescription says the exact same milligrams from one month to the next, the units, or volume, you draw up in your syringe could be completely different. Same dose on paper. Completely different injection in reality.
That’s exactly how dosing errors happen.
Different concentrations. Same prescription. This is what pharmacy hopping actually looks like.
What the FDA Is Actually Saying About This
This isn’t just my opinion as a nurse. The FDA has been raising the alarm on compounded GLP-1 safety for a while now.
As of April 2025, the FDA had received over 500 adverse event reports related to compounded semaglutide and nearly 500 reports concerning compounded tirzepatide. And that number is almost certainly higher because most state-licensed compounding pharmacies aren’t even required to submit adverse event reports.
The FDA has received multiple reports of adverse events, some requiring hospitalization, linked to dosing errors associated with compounded injectable semaglutide. These weren’t errors because people were careless. Many of them were errors because the concentration changed, and nobody clearly explained that.
The FDA estimates that 10 deaths and 100 hospitalizations may be linked to the use of compounded GLP-1 medications. And their responses are often reactive, meaning action is usually taken only after something has already gone wrong.
That last part is the part that keeps me up at night as a nurse.
A Real Example of What Can Go Wrong
I know someone personally who accidentally took four times her dose. Four times. It happened because her pharmacy changed, and she drew up the volume exactly the same as what she was used to… but the concentration was completely different. She felt absolutely awful.
And here’s the thing that really got me. I’m a NICU nurse. Dosage calculations are literally what I do every single day. Tiny babies depend on my accuracy. And I STILL panicked after my own pharmacy changed. I had to go back to my written notes to confirm I’d taken the right dose. I had gone over it so many times in my head that I couldn’t remember what I’d actually done.
If it can happen to me… it can happen to anyone.
Same medication. Different pharmacy. Different concentration. This is exactly what pharmacy hopping looks like in real life.
What to Look For in a Compounded GLP-1 Provider
Not all telehealth companies operate the same way. Here’s what actually matters when it comes to safety:
Pharmacy consistency. Your medication should come from the same pharmacy every single month. No exceptions. If your provider can’t tell you exactly which pharmacy fills your prescription, that’s a red flag worth paying attention to.
Standardized dosing. As your dose increases, your units should stay the same. Simple, consistent, easy to follow instructions reduce the risk of errors. If the math changes every time your dose changes, that’s unnecessary confusion and unnecessary risk.
Transparency. A trustworthy provider will tell you where your meds come from, how they’re compounded, and what quality standards their pharmacy follows. You have every right to ask those questions.
Why I Made the Switch
This is a big part of why I moved to EllieMD. One pharmacy, always the same one, every single month. Standardized dosing so the units stay consistent no matter what milligram you’re on. Simple. Clear. And a whole lot less room for the kind of errors that send people to the hospital.
This is what consistency looks like. Same pharmacy. Every single month.
Questions to Ask Your Telehealth Provider Right Now
Before your next injection, it’s worth picking up the phone or sending a message to ask:
Where is my prescription being filled? Is it always the same pharmacy? How is my dosing calculated and does that change if my concentration changes? What quality standards does your compounding pharmacy follow?
You deserve clear answers. If you’re not getting them, that tells you something too.
This post contains affiliate links and/or brand partnership content. I may earn a commission at no extra cost to you.
LET’S BE CLEAR ABOUT WHO I AM (AND WHO I’M NOT).
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing on this site replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
SCOPE OF PRACTICE.
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment — this is not something that should be DIY’d. These statements have not been evaluated by the FDA. Products discussed on this site are not intended to diagnose, treat, cure, or prevent any disease.
TRANSPARENCY.
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links on this site are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate I earn from qualifying purchases.
RESULTS + TESTIMONIALS.
Any testimonials or results shared on this site reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
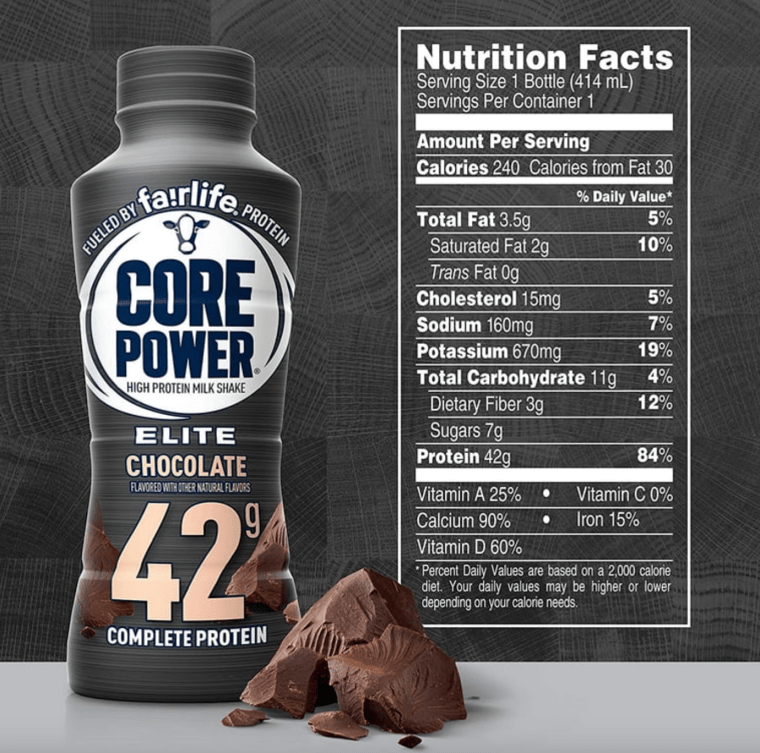
After losing 94 pounds, I’ve learned a few things about protein.
Some protein is actually good. Some is… questionable. And some makes you pause mid-sip and think, wait. Was that even protein???
For a long time, I thought protein was mostly for gym bros trying to bulk up & flex in the mirror. You know the vibe. Giant tubs. Aggressive labels. Shakers that smell suspicious even after washing.
Turns out, protein is way more important than I ever realized, especially during weight loss.
Why protein matters way more than you think
Protein isn’t about getting huge. It’s about protecting what you already have.
When you’re losing weight, especially if you’re in a calorie deficit, your body doesn’t just burn fat. It also breaks down muscle if it doesn’t have enough protein to work with. And muscle matters more than people realize.
Muscle helps keep your metabolism humming. Less muscle can mean a slower metabolism, lower energy, and weight loss that feels harder and harder to maintain.
Protein helps prevent that. It gives your body the building blocks it needs to repair and rebuild instead of breaking things down.
It also keeps you full longer. Not “I just ate and I’m still thinking about snacks” full. Actual, satisfied, walk-away-from-the-pantry full.
And yes, it supports your metabolism even when you’re doing very important activities like sitting on the couch scrolling TikTok.
The nerdy nurse explanation you didn’t get in health class.
When calories drop, your body looks for fuel. Fat is one source. Muscle is another. If protein intake is too low, muscle loss happens faster. That muscle loss can slow your metabolism, which makes continued weight loss and maintenance harder over time.
Protein helps signal to your body, hey, we need this muscle. Please don’t toss it.
This is especially important if you’re losing weight with medication, lifestyle changes, or a combination of both. The goal isn’t just a smaller number on the scale. It’s feeling strong, energized, and able to keep the results long-term.
Not all protein is created equal
Just because something says “high protein” on the label does not mean it’s doing anything helpful for your body. Some options are high quality and easy to absorb. Others are basically flavored air with a side of digestive regret.
Over the past couple years, I’ve tried a lot. Powders. Ready-to-drink shakes. Bars. And a few things that can only be described as science experiments that should’ve stayed on the shelf.
Some tasted fine but didn’t keep me full. Some had great macros but wrecked my stomach. Some were so chalky they made me question my life choices.
Through trial, error, and a whole lot of label reading, I’ve figured out which ones are actually worth your time. Not perfect. Not magic. Just solid options that taste decent, digest well, and actually support a weight loss journey.
So what should you look for?
You don’t need perfection. You need consistency.
A protein source that:
Keeps you full longer
Doesn’t upset your stomach
Fits into your real life, not an influencer meal plan
Helps you hit your daily protein without feeling like a chore
Protein should make your life easier, not more complicated.
Professional Disclosure: I provide BS-free metabolic education as a registered nurse and health coach for women navigating PCOS, perimenopause, and stubborn weight loss. While I share evidence-based research and nurse-informed support, please remember that I am not your nurse. The content shared here is for educational purposes only. It does not constitute medical advice, diagnosis, or treatment, and it does not establish a provider-patient relationship. Nothing on this site is a substitute for care from a licensed provider who knows your full health history. All opinions and content shared on this platform are my own and do not reflect the views or endorsements of my employer or the hospital where I am employed.
Scope of Practice and FDA: Per professional coaching guidelines, I may recommend over the counter (OTC) medications or supplements to support your wellness goals. However, I do not prescribe or recommend specific prescription medications. For prescription options, including GLP-1 tools, my role is to help you understand the available science so you can have an informed discussion with your licensed healthcare provider. These statements have not been evaluated by the Food and Drug Administration. Products discussed are not intended to diagnose, treat, cure, or prevent any disease, and medical treatments require professional oversight.
Trust and Transparency: I only recommend products I trust. Most are items I use personally, while others are shared based on my professional trust in the clinical standards of partners like Ellie MD. Some links are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate I earn from qualifying purchases.