I saw the new KLOW blend and was immediately like… hold up, wait a minute.
This has the GHK-Cu that I already LOOOOOVE, plus the BPC-157/TB-500 I had already been contemplating adding… ANNNND the KPV all in one?
Hell yes, sign me up.
If you’ve been around here for more than five minutes, you already know I’m not just casually curious about GHK-Cu. I’m on it. I love it. I have been very impressed by it. I’ve had more new baby hairs with GHK-Cu than I’ve seen with anything else I’ve tried in the last 10 years. My hair is growing faster, and I’ve also noticed improvement in the loose skin on my arms and neck.
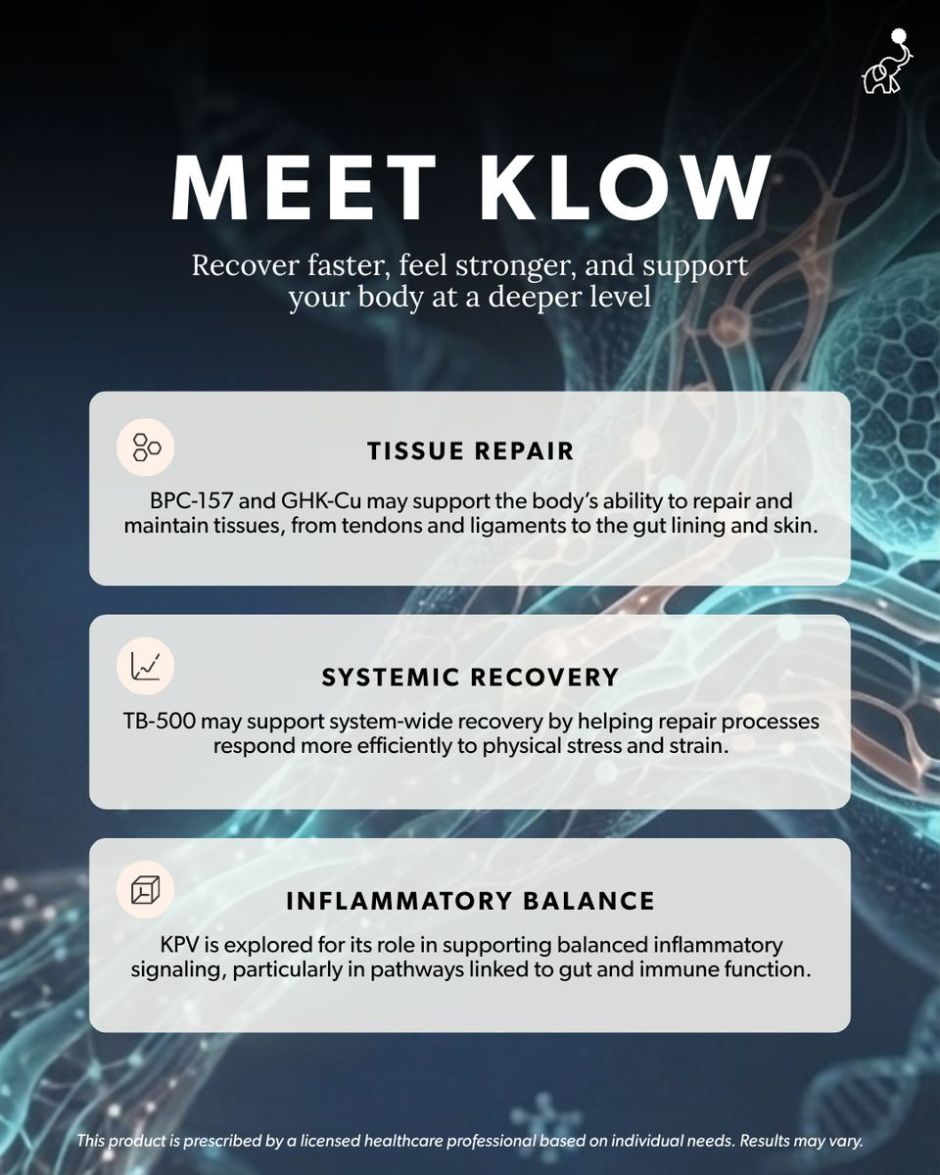
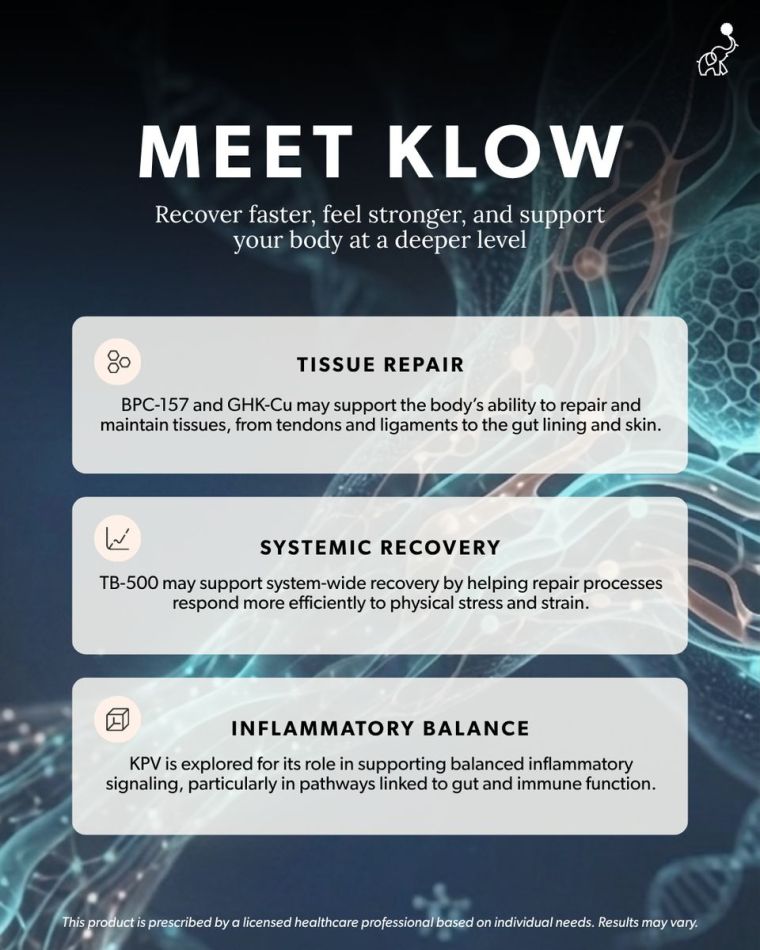
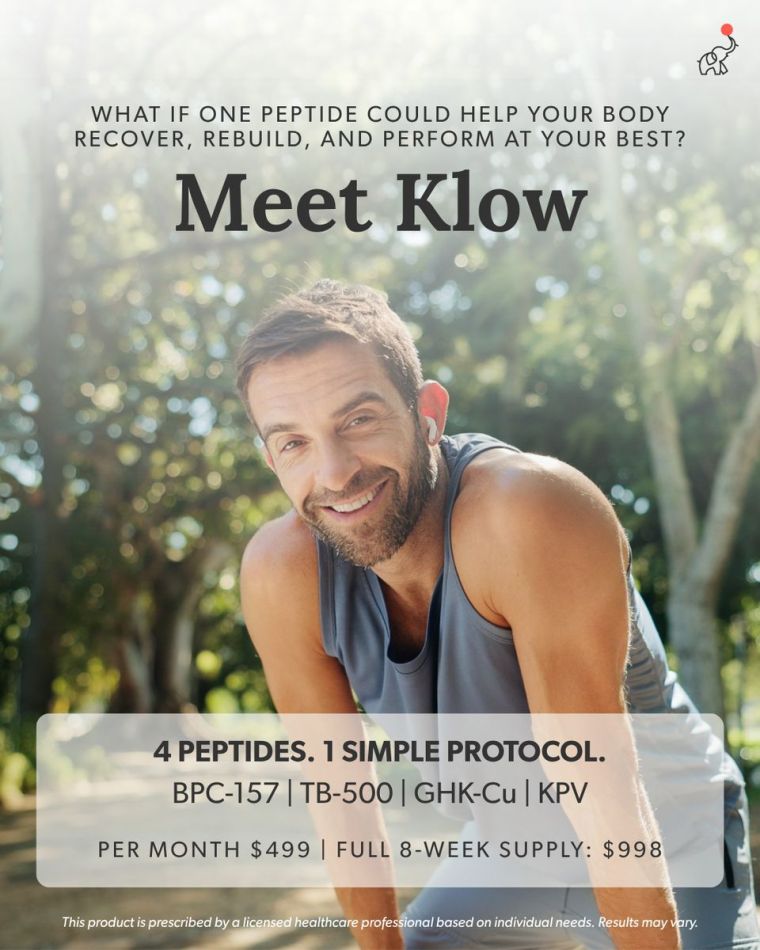
So when I saw that EllieMD released a new compounded peptide blend with GHK-Cu in it, I wanted the details immediately. Then I realized it also includes BPC-157/TB-500, which I had already been looking at for recovery and tissue support, plus KPV, which I’ve been curious about for gut and inflammatory balance. It brings together several peptides I was already looking into separately, especially for the stuff so many of us start caring about when our bodies stop bouncing back like they used to…
Skin changes. Recovery. Gut support. Inflammation. Collagen. The “why do I feel like my body needs a system update?” era.
KLOW is one I would absolutely want to know about if you’ve been curious about peptides beyond GLP-1s, especially if you’re thinking more about long-term wellness, recovery, and supporting what your body is already trying to do.
CHECK OUT KLOW HERE
If you’ve clicked a link and can’t see KLOW, it’s because it’s one that requires Exclusive Access to view. Just sign in with your free EllieMD account
OR CREATE ONE HERE
XOXO, NIKI
PCOS. Perimenopause. Metabolic health. The real stuff. Not just “eat less, move more.”
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing here replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
Scope of practice
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment. These statements have not been evaluated by the FDA. Products discussed are not intended to diagnose, treat, cure, or prevent any disease.
Transparency
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links in this email are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate, I earn from qualifying purchases.
Results + Testimonials
Any testimonials or results shared here reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
Can I tell you the thing that still makes me want to flip a table?
It’s the phrase “your labs are normal.”
Because for a lot of women… especially women with PCOS, perimenopause knocking, and years of “borderline” results that nobody ever actually addressed… “normal” doesn’t mean fine. It means nobody looked deep enough.
Here’s what most routine bloodwork checks when it comes to blood sugar: fasting glucose and A1C. That’s it.
And here’s what those tests miss: how hard your body is working to keep those numbers where they are.
Your fasting glucose could be sitting at a perfect 94 mg/dL. Your A1C could be a beautiful 5.4%. And your pancreas could be GRINDING out insulin behind the scenes just to hold those numbers in place. You wouldn’t know. Because nobody ordered the test that shows it.
That test is called fasting insulin. And when you pair it with your fasting glucose, you can calculate something called your HOMA-IR score… which basically tells you how insulin resistant your body is right now.
Not how your blood sugar looks on paper. How your body is actually functioning.
The CDC says over 115 million American adults have prediabetes. 8 in 10 don’t know it. That’s not because they’re ignoring their health. It’s because the standard tests aren’t catching it early enough.
And research published in Diabetes Care found that using A1C alone to screen for prediabetes missed about 75% of at-risk people.
If that doesn’t make you want to flip the table too… I don’t know what will.
Here’s what I want you to do:
Next time you have bloodwork, ask your doctor to add a fasting insulin level. It’s drawn from the same blood, at the same time. You may need to specifically request it because it’s not included in standard panels.
Once you have it, here’s the math: (fasting glucose x fasting insulin) / 405 = your HOMA-IR score. Under 1.0 = optimal. Over 2.5 = insulin resistance may be present. Over 3.0 = significant.
That one number could explain more about why you feel the way you feel than every “normal” result you’ve ever gotten combined.
I wrote a full deep dive on this on the blog… why standard panels miss it, what it means if you have PCOS, and the exact labs I’d tell my best friend to ask for. If you want the whole picture, it’s there for you.
Not sure where to start? Take my free quiz and I’ll send you a custom plan.
WHAT’S RIGHT FOR MY BODY?
P.S. Missed the previous editions of The Nurse’s RX? ↓ Catch up here ↓
READ PAST EDITIONS
↓ LET’S CONNECT ↓
Let’s be clear about who I am (and who I’m not)
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing here replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
Scope of practice
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment. These statements have not been evaluated by the FDA. Products discussed are not intended to diagnose, treat, cure, or prevent any disease.
Transparency
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links in this email are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate, I earn from qualifying purchases.
Results + Testimonials
Any testimonials or results shared here reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
One of the first things people notice is that it can turn your urine blue or blue-green. But don’t panic, it’s not dangerous. It’s actually a sign your body is processing it the way it should. Your body uses what it needs and gets rid of the rest.
Nowww… if your 💩 turns blue?
Different conversation. That’s when you reach out to your provider. That plot twist may mean that methylene blue isn’t being broken down in your body the way we want it to.
Methylene blue itself isn’t new at all. It’s a pharmaceutical-grade compounded dye that’s been used in medicine for over 150 years. Hospitals were using it long before wellness trends were even a thing. The version we offer is prescribed and overseen by licensed medical providers, not something pulled from a supplement aisle or online marketplace.
She’s the OG. Truly.
What’s new is the interest in how low doses of methylene blue may support focus, mental clarity, and steadier energy. Especially during seasons like perimenopause, when energy doesn’t feel predictable anymore and brain fog shows up uninvited.
This isn’t a stimulant.
Think less caffeine spike and more steady support. Like a slow, continuous IV infusion instead of a quick IV bolus. No jitters. No crash.
A lot of the conversation around methylene blue centers on cellular energy, which is really just how efficiently your cells turn oxygen and nutrients into usable energy. When that process slows down, it doesn’t always feel like sleepiness. It often shows up as true mental fatigue, low motivation, or that mid-day crash coffee can’t fix.
There are studies that have suggested methylene blue may play a role in long term brain health and cognitive function, which is why it’s entered the Alzheimer’s conversation. One thing that doesn’t get talked about much is that long-term studies with methylene blue are hard to keep truly “blind.” When something can turn your urine blue, participants and researchers can usually tell who’s taking it, which makes long-term data harder to interpret.
That’s part of why methylene blue keeps getting studied… and also why the conversation around it stays nuanced.
Methylene blue is being studied for its potential role in supporting cognitive function, cellular energy, and mitochondrial health.
Did I mention our version is a pill, not an injection??? Yep.
So if you’ve wanted to support your energy, focus, and brain health, but didn’t want injections at all… or don’t want to add yet another injection to your stack… you may loooove this little blue pill.
More to come on this one, because the questions around it keep rolling in.
Not sure where to start? Take my free quiz and I’ll send you a custom plan.
WHAT’S RIGHT FOR MY BODY?
P.S. Missed the previous editions of The Nurse’s RX? ↓ Catch up here ↓
READ PAST EDITIONS
↓ LET’S CONNECT ↓
Let’s be clear about who I am (and who I’m not)
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing here replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
Scope of practice
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment. These statements have not been evaluated by the FDA. Products discussed are not intended to diagnose, treat, cure, or prevent any disease.
Transparency
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links in this email are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate, I earn from qualifying purchases.
Results + Testimonials
Any testimonials or results shared here reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
You leave your doctor’s appointment with the same answer you’ve gotten for the last five years. “Everything looks good. Labs are normal.”
And you sit in your car and think… then why do I feel like this? Why am I exhausted by 2pm every day? Why can’t I lose weight no matter what I do? Why does my brain feel like it’s running through fog? Why am I doing everything “right” and nothing is changing?
You’ve heard “your labs are normal” so many times that you’ve started to believe the problem must be you. Your discipline. Your effort. Your willpower.
It’s not you. And I need you to hear that.
Your labs might technically be within range. But “within range” and “optimal” are not the same thing. And the test that would actually tell you whether you have insulin resistance? There’s a very good chance your doctor never ordered it.
What Is a Fasting Insulin Test and Why Don’t Most Doctors Order It?
When you go in for your annual physical or routine bloodwork, your doctor typically checks two things related to blood sugar: your fasting glucose and your A1C (hemoglobin A1C).
Fasting glucose is a snapshot. It tells you what your blood sugar is right now, after you haven’t eaten for 8 to 12 hours. A result under 100 mg/dL is considered normal. Between 100 and 125 is prediabetes. Over 126 is diabetes.
A1C is a wider view. It measures your average blood sugar over the last 2 to 3 months by looking at how much sugar has attached to your red blood cells. Under 5.7% is normal. 5.7 to 6.4% is prediabetes. Over 6.5% is diabetes.
Both of these tests measure the same thing… glucose. They just measure it differently.
And here’s the problem: neither one tells you how hard your body is working to keep that glucose number “normal.”
Think of it this way. Imagine two women sitting in the same doctor’s office on the same day. Both have a fasting glucose of 94 mg/dL. Both A1Cs come back at 5.4%. Both get told their labs are normal.
But behind the scenes, the first woman’s pancreas is producing 5 units of insulin to maintain that glucose level. Easy. No sweat. Her metabolic system is cruising.
The second woman’s pancreas is grinding out 18 units of insulin just to hold the line at 94. Her body is working triple shifts to keep that number where it is. She’s exhausted, gaining weight she can’t explain, brain fog is constant, and she can’t stop thinking about food.
On paper, they look identical. Metabolically, they’re in completely different places.
The only way to see the difference? A fasting insulin test. And most routine bloodwork panels do not include it.
That’s not an oversight by your specific doctor. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) states plainly that doctors use blood tests to find out if someone has prediabetes, but they don’t usually test for insulin resistance. It’s just not part of the standard protocol. Which means millions of women are walking around with insulin resistance that nobody is looking for… because nobody is ordering the test that would find it.
What Is HOMA-IR and How Do You Calculate It?
A fasting insulin test measures how much insulin your pancreas is producing after you haven’t eaten. That number alone is helpful. But when you combine it with your fasting glucose, you can calculate something even more useful… your HOMA-IR score (Homeostatic Model Assessment of Insulin Resistance). This is essentially a number that tells you how insulin-resistant your body is.
The math is simple: (fasting glucose x fasting insulin) / 405.
Both values must come from the same fasting blood draw.
Here’s how to read your HOMA-IR score: Under 1.0 — Optimal insulin sensitivity. Your body is using insulin efficiently. 1.0 to 2.5 — Moderate range. Worth watching, especially if you have other risk factors like PCOS, family history of diabetes, or unexplained weight gain. Over 2.5 — Insulin resistance is likely present. Your pancreas is working harder than it should to keep your blood sugar in range. Over 3.0 — Significant insulin resistance. This level may already be driving symptoms… fatigue, weight gain, brain fog, food noise… even if your glucose and A1C still look completely normal on paper.
So why doesn’t your HOMA-IR show up on your standard bloodwork? A few reasons. Most standard metabolic panels are built around glucose, not insulin. Time constraints in a 15-minute appointment don’t leave room for expanded testing. And many providers follow a “wait and see” approach to borderline results… meaning they don’t dig deeper until your numbers actually cross into prediabetes or diabetes territory.
By then, the damage has been building for years.
Can You Have Insulin Resistance with Normal Blood Sugar and a Normal A1C?
Yes. And this is the part that makes me want to flip a table.
Your fasting glucose can be perfect. Your A1C can be textbook. And insulin resistance can still be building behind the scenes for years because your pancreas is compensating… producing more and more insulin to keep your blood sugar in range.
According to the Cleveland Clinic, as long as your pancreas can make enough insulin to overcome the resistance, your blood sugar levels will stay in a healthy range and you won’t have any symptoms. But over time, the cells that make insulin can wear out. That’s when blood sugar finally rises. That’s when you get the prediabetes or diabetes diagnosis. But the insulin resistance? That started long before the numbers changed.
Research from a peer-reviewed study published in a PMC journal found that elevated insulin levels in the absence of impaired glucose tolerance and normal A1C may actually be a much earlier indicator of metabolic disease risk than glucose or A1C alone. In other words… insulin was waving a red flag the whole time. Nobody was watching for it.
How Many People Have Undiagnosed Insulin Resistance and Prediabetes?
According to the CDC’s most recent National Diabetes Statistics Report (January 2026), over 115 million American adults have prediabetes. And 8 in 10 of them don’t know it.
Let that sink in for a second. 80% of people with prediabetes are walking around right now being told their labs are normal.
On top of that, research published in Diabetes Care found that using A1C alone to screen for prediabetes missed about 75% of at-risk individuals. The study specifically noted that A1C was less sensitive for detecting at-risk individuals compared to fasting glucose and glucose tolerance testing… and none of those tests even measure insulin.
Meanwhile, a growing body of research shows that elevated insulin levels can appear years… and according to some researchers, potentially even decades… before blood sugar ever crosses into an abnormal range. Your pancreas is working overtime to keep your glucose normal, and nobody’s checking to see how hard it’s working.
Why Insulin Resistance Testing Matters Even More If You Have PCOS
If you have polycystic ovary syndrome, this isn’t just relevant. It may be the entire missing piece of your health puzzle.
Research estimates that insulin resistance affects between 50 and 80% of women with PCOS… including women who are not overweight. That’s not a small subset. That’s the majority. And many of those women have never had their insulin levels checked.
Insulin resistance in PCOS doesn’t just affect blood sugar. It directly drives excess androgen (testosterone) production, which can cause irregular periods, acne, hair loss, excess body hair, and difficulty getting pregnant. The cycle looks like this: insulin resistance leads to higher insulin levels, which triggers increased androgen production, which disrupts ovulation, which worsens PCOS symptoms. It feeds itself.
And the whole time, your fasting glucose and A1C may look completely normal because your pancreas is compensating.
One peer-reviewed study in the Journal of Clinical Medicine proposed that the medical community needs to shift from a “glucose-centric” approach to an “insulin-centric” model when managing PCOS… because by the time glucose rises, the metabolic damage has already been happening for years. The study emphasized that early identification of insulin resistance would enable timely intervention and could reduce the risk of long-term metabolic and reproductive complications.
If you’ve been told your labs look fine but you’re still gaining weight, still exhausted, still struggling with PCOS symptoms that nobody can explain… this may be why. The right labs were never ordered.
What Blood Tests Should You Ask Your Doctor For?
Ask for a fasting insulin test at your next appointment.
It’s a simple blood draw done at the same time as your regular fasting labs.
You may need to specifically request it… many providers won’t think to order it unless you ask.
If your provider pushes back, you can explain that you’d like to assess insulin resistance beyond what glucose and A1C alone can show.
The NIDDK confirms that providers don’t usually test for insulin resistance as part of standard screening.
That doesn’t mean the test isn’t available or valuable. It means you may need to advocate for yourself.
Know your HOMA-IR score.
Once you have your fasting insulin and fasting glucose from the same blood draw, you can calculate it yourself:
(fasting glucose x fasting insulin) / 405.
Under 1.0 is optimal.
Over 2.5 starts to suggest insulin resistance.
Over 3.0 is significant.
There are also free HOMA-IR calculators online if math isn’t your thing.
Ask about a full hormone panel if you have PCOS or suspect it.
Fasting insulin
HOMA-IR
testosterone (total and free)
DHEA-S
LH
FSH
lipid panel
These give a much more complete picture of what’s happening metabolically and hormonally than glucose and A1C alone.
Know the difference between “normal range” and “optimal.”
Lab reference ranges are based on population averages… they tell you where most people fall, not where you should be for your best health.
A fasting glucose of 98 is technically “normal” but it’s not optimal.
An A1C of 5.6 is technically “normal” but it’s one decimal point from a prediabetes diagnosis.
Don’t let “in range” make you stop asking questions.
Trust your body.
If you feel like something is off, something probably is.
I was the woman in the car. I had PCOS. I had high blood pressure, high cholesterol, and sleep apnea. I was labeled pre-diabetic for about eight months in 2006… and then my A1C came back down and everybody moved on. Normal. Case closed.
Except my white blood cell count kept showing chronic inflammation. Nobody connected those dots. Nobody said “hey, your A1C looks better but let’s dig deeper into WHY your body is still inflamed, WHY you can’t lose weight, WHY none of this is adding up.”
I never got the right tests. I still haven’t. What I got was a doctor who finally looked at me and said… something isn’t adding up. The calories in versus calories out math wasn’t mathing. My body wasn’t responding the way it should have been. And instead of handing me another pamphlet, he prescribed a GLP-1.
That changed everything. But I think about how many years I spent blaming myself for something that had a physiological explanation nobody bothered to look for. How many times I white-knuckled a diet and watched the scale not move and thought it was ME.
I’m a NICU nurse. I believe in evidence. I believe in labs. But I also believe that the wrong labs… or the incomplete ones… can leave you blaming yourself for something that was never your fault.
If your doctor says your labs are normal but your body is screaming that something is wrong… believe your body. Then go get the right labs. The ones I’m telling you about in this post? I wish someone had told me about them ten years ago.
Frequently Asked Questions About Insulin Resistance and Lab Testing
Can you have insulin resistance with a normal A1C?
Yes. Insulin resistance can develop years before your A1C ever moves out of the normal range. Your pancreas compensates by producing more insulin to keep blood sugar stable. As long as it can keep up, your glucose and A1C may look fine on paper while insulin resistance builds underneath. A fasting insulin test or HOMA-IR calculation can reveal what glucose-based tests miss.
What is HOMA-IR and how do I get tested?
HOMA-IR stands for Homeostatic Model Assessment of Insulin Resistance. It’s not a separate blood test… it’s a calculation using two values from a single fasting blood draw: your fasting glucose and your fasting insulin. The formula is (fasting glucose x fasting insulin) / 405. A score under 1.0 is considered optimal. Over 2.5 suggests insulin resistance. Over 3.0 is significant. You’ll need to ask your doctor to order a fasting insulin level since it’s not included in standard metabolic panels.
Does a normal fasting glucose mean I don’t have insulin resistance?
Not necessarily. Your fasting glucose measures what your blood sugar is at one moment in time. It doesn’t tell you how much insulin your body needed to get it there. Two people can have the exact same fasting glucose but very different insulin levels… and very different levels of metabolic stress happening behind the scenes.
Why doesn’t my doctor test for insulin resistance?
Most standard bloodwork panels focus on glucose, not insulin. The NIDDK notes that providers don’t usually test for insulin resistance as part of routine screening. It’s not that the test doesn’t exist or isn’t valuable. It’s that the current standard of care doesn’t include it unless you specifically ask or your provider is thinking beyond the basics.
What blood tests should I ask for if I have PCOS?
For a more complete metabolic and hormonal picture, consider asking about: fasting insulin, fasting glucose (to calculate HOMA-IR), A1C, testosterone (total and free), DHEA-S, LH, FSH, and a full lipid panel. These tests together can reveal insulin resistance, hormonal imbalances, and metabolic risk factors that glucose and A1C alone would miss.
Is it too late to test for insulin resistance in my 40s?
No. Research shows that lifestyle and medical interventions can reduce the risk of progressing from insulin resistance to type 2 diabetes significantly… even in midlife. The earlier you identify insulin resistance, the more options you have. But “earlier” doesn’t mean it has to be your 20s. It means earlier than waiting for a diabetes diagnosis.
Not sure where to start? My free Wellness Strategy Quiz can help you figure out what to focus on first based on where you are right now
Lorenzo C, et al. “A1C Between 5.7 and 6.4% as a Marker for Identifying Pre-Diabetes, Insulin Sensitivity and Secretion, and Cardiovascular Risk Factors.” Diabetes Care. 2010;33(9):2104-2109.
Parker J. “Recognizing the Role of Insulin Resistance in Polycystic Ovary Syndrome: A Paradigm Shift from a Glucose-Centric Approach to an Insulin-Centric Model.” Journal of Clinical Medicine. 2025;14(12):4021.
“Hyperinsulinemia: An Early Biomarker of Metabolic Dysfunction.” PMC. 2023. pmc.ncbi.nlm.nih.gov/articles/PMC10186728
Cleveland Clinic — Insulin Resistance: What It Is, Causes, Symptoms & Treatment — my.clevelandclinic.org/health/diseases/22206-insulin-resistance
“Markers of Insulin Resistance in Polycystic Ovary Syndrome Women: An Update.” World Journal of Diabetes. 2022. pmc.ncbi.nlm.nih.gov/articles/PMC8984569
“Insulin Resistance, Metabolic Syndrome and Polycystic Ovaries: An Intriguing Conundrum.” Frontiers in Endocrinology. 2025.
Ezeh U, et al. “Detecting Insulin Resistance in Polycystic Ovary Syndrome: Purposes and Pitfalls.” PubMed. 2004.
This site contains affiliate links and/or brand partnership content. I may earn a commission at no extra cost to you.
LET’S BE CLEAR ABOUT WHO I AM (AND WHO I’M NOT).
I’m a registered nurse and health coach who shares real, BS-free information about metabolic health, PCOS, perimenopause, and weight loss, because y’all deserve better than vague wellness fluff. But here’s what I need you to know: I am not YOUR nurse. Everything I share here is for educational purposes only. It is not medical advice, it’s not a diagnosis, and it doesn’t create a provider-patient relationship between us. Nothing on this site replaces the care of a licensed provider who actually knows your full health history. The opinions and content here are my own and do not reflect the views of my employer or the hospital where I work.
SCOPE OF PRACTICE.
As a nurse health coach, I can recommend over-the-counter products and supplements that may support your wellness goals. I don’t prescribe specific prescription medications. When it comes to GLP-1s and peptides, what I can do is talk about the science, what’s available, and what may be beneficial, so you can have an informed conversation with your licensed medical provider. The decision about what’s right for your body always belongs to you and your provider. Always consult your licensed provider before starting any prescription treatment — this is not something that should be DIY’d. These statements have not been evaluated by the FDA. Products discussed on this site are not intended to diagnose, treat, cure, or prevent any disease.
TRANSPARENCY.
I only recommend things I actually trust. Most are products I personally use, some are from partners whose clinical standards I believe in. I will always let you know when it’s something I haven’t tried personally. Some links on this site are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate I earn from qualifying purchases.
RESULTS + TESTIMONIALS.
Any testimonials or results shared on this site reflect individual experiences only. Results are not guaranteed and will vary based on individual circumstances.
Summer is fast approaching, and if I’m being totally honest, a couple of years ago that thought would have sent me into a literal panic.
I used to dread this season. There were summers when I didn’t even own a bathing suit that fit. I refused to buy shorts because I was so uncomfortable in my own skin. Instead, I lived in long dresses and leggings because they felt “safer” and more hidden, even in the middle of a Southern heatwave.
192 lbs and right on the edge of a total life change. This was the moment I stopped making excuses.
Pool invites? They stressed me out. Beach trips? They felt exposing and exhausting. And photos? Absolutely not. I was the queen of hiding in the back or offering to be the one taking the picture so I didn’t have to be in it.
The Willpower Myth
For years, I kept telling myself I just needed more discipline. I thought I needed more willpower or maybe just one more “perfect” fad diet to finally see results. So, I did what we all do. I counted every single calorie. I tracked every tiny bite. I tried whatever new trend was blowing up on social media that month.
And every time it didn’t “stick,” I blamed myself. I felt like a failure because my “math wasn’t mathing” no matter how hard I worked.
Upgrading the Strategy
What actually changed everything for me? I stopped fighting my biology and started upgrading my strategy.
I stopped counting calories. No more obsessing over every number.
I started eating intelligently. I focused on Protein first and Fiber daily (IYKYK 💩).
The “Food Noise” quieted. My body finally had the metabolic support it was screaming for.
Everything fell into place. My health risks vanished and my energy came back.
A Whole New View
This past summer? Things looked a lot different. I actually had a whole drawer of bathing suits. An actual drawer! And yes, a whole drawer of shorts too.
Living my life again at 115 lbs! I finally have the energy and confidence to show up for every moment.
That didn’t come from “trying harder” or white-knuckling my way through another restrictive meal plan. It came from finally giving my body the tools it needed to succeed.
Summer is coming either way, sis. You get to decide how you walk into it this year. Are you going to be hiding in the back, or are you ready to finally feel like the main character of your own life?
Ready to make this your best summer yet?
If you are exhausted from fighting your own biology, let’s chat! You don’t have to do this alone.
Want a personalized plan? Let me help you create the best wellness strategy to fit your needs. TAKE MY QUIZ NOW or if you’d prefer to talk to me on the phone CLICK HERE TO BOOK A FREE 15 MIN CALL WITH ME
Let’s talk through your concerns and see if this path is right for you! Or, you can GET STARTED THROUGH MY SITE if you already know you’re ready to see your own math finally math, let’s go!
☀️ My “Main Character” Summer Essentials Checklist
If you are ready to stop hiding in the leggings and start enjoying the sunshine, here is what is in my beach bag this season. These are my non-negotiables for staying energized and feeling like a 10/10 while I’m out and about!
The Perfect Summer Sip: A crisp Diet Cherry Coke or a refreshing Alani Nu (I’m currently reaching for the fruitier flavors to match the vibe). It’s all about that bubbly energy without the sugar crash!
The “Confidence” Romper: You saw the pink romper! My summer essential is having at least one outfit that makes me feel absolutely radiant. No more “safe” long dresses for this girl!
My Ellie MD Support: I never go into a new season without checking in with my team. Having that metabolic support means I can enjoy the summer without the “math isn’t mathing” stress.
Professional Disclosure: I provide BS-free metabolic education as a registered nurse and health coach for women navigating PCOS, perimenopause, and stubborn weight loss. While I share evidence-based research and nurse-informed support, please remember that I am not your nurse. The content shared here is for educational purposes only. It does not constitute medical advice, diagnosis, or treatment, and it does not establish a provider-patient relationship. Nothing on this site is a substitute for care from a licensed provider who knows your full health history. All opinions and content shared on this platform are my own and do not reflect the views or endorsements of my employer or the hospital where I am employed.
Scope of Practice and FDA: Per professional coaching guidelines, I may recommend over the counter (OTC) medications or supplements to support your wellness goals. However, I do not prescribe or recommend specific prescription medications. For prescription options, including GLP-1 tools, my role is to help you understand the available science so you can have an informed discussion with your licensed healthcare provider. These statements have not been evaluated by the Food and Drug Administration. Products discussed are not intended to diagnose, treat, cure, or prevent any disease, and medical treatments require professional oversight.
Trust and Transparency: I only recommend products I trust. Most are items I use personally, while others are shared based on my professional trust in the clinical standards of partners like Ellie MD. Some links are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate I earn from qualifying purchases.
Tired of Running on Empty? The Cellular Key to Boosting Metabolism & Focus
That Energy Drink Crash is NOT Normal
You ever hit the point where your third Alani just feels like a very expensive can of fizzy disappointment? Were you relying on that quick jolt to get you through your day (or night if you’re like me), but the energy part packed up and left the building? SAME SIS, SAME!
That crashing feeling, that chronic metabolic fatigue, isn’t just about poor habits. The truth is, it might be a shortage of a critical molecule your body needs to function at its peak.
NAD+ is basically the MVP molecule that helps your body turn food into actual, usable energy. Think of NAD+ as the spark plug for your cellular engine. You need a strong spark to ignite your fuel and get moving. The studies show that NAD+ helps keep your cells young and resilient and improves how your body’s Energy Factory works, which is the heart of your energy production. For me, it was like the five thousand tabs in my brain finally closed themselves.
It keeps everything running smoothly:
Focus
Metabolism
Mood
The Spark Plug runs all of it. When the spark plug is weak, every system reading, from your energy output to your focus, is compromised.
NAD+ is a vital coenzyme for cellular health. Learn how Ellie MD’s NAD+ formulation can help support your energy production, DNA repair, and overall metabolic function.
The Metabolic Stressors Aging Your Energy
So if NAD+ is so critical for cellular energy, why do we constantly feel so depleted?
NAD+ levels drop as we age. This is unavoidable. But those levels also drop due to chronic stress or when we are running on caffeine and vibes. You are surviving on pure grit, and your brain literally feels like TV static.
In my own experience, this is where I saw the biggest win. That overwhelming, chaotic ADHD haze I used to deal with started easing up; it was like the five thousand tabs stuck open in my brain finally closed themselves instead of crashing. I felt clearer and more “with it.”
The Glow Up is Real (Even the Awkward Part)
NAD+ plays a major role in cellular energy and turnover, which is great for your skin. I can tell you that my skin definitely had its own little purge moment at first—hello, surprise zits! But that initial reaction can be a normal part of the process.
Once that purge was over? Game changer. People were literally giving me compliments and asking what foundation I was wearing because my skin looked so good—and I wasn’t even wearing any! That’s when I knew the NAD+ was doing the dang thing and the cell turnover was happening!
The Difference Between Dragging and Doing
Supporting those NAD+ levels can help your body’s natural energy process stay on track. It’s not a miracle fix or a sudden jittery jolt; it’s a subtle, steady kind of clarity that coffee wishes it could give.
If you’re curious about the next-level science on cellular maintenance and DNA repair benefits of NAD+ that weren’t covered here, I have an exclusive NAD+ 101 note that is just for you!
To receive the NAD+ 101 Note
drop a comment below
or Text Me
P.S. If this post helped you finally understand your energy crash, share it with a friend who is also tired of relying on that third can of Alani!
Professional Disclosure: I provide BS-free metabolic education as a registered nurse and health coach for women navigating PCOS, perimenopause, and stubborn weight loss. While I share evidence-based research and nurse-informed support, please remember that I am not your nurse. The content shared here is for educational purposes only. It does not constitute medical advice, diagnosis, or treatment, and it does not establish a provider-patient relationship. Nothing on this site is a substitute for care from a licensed provider who knows your full health history. All opinions and content shared on this platform are my own and do not reflect the views or endorsements of my employer or the hospital where I am employed.
Scope of Practice and FDA: Per professional coaching guidelines, I may recommend over the counter (OTC) medications or supplements to support your wellness goals. However, I do not prescribe or recommend specific prescription medications. For prescription options, including GLP-1 tools, my role is to help you understand the available science so you can have an informed discussion with your licensed healthcare provider. These statements have not been evaluated by the Food and Drug Administration. Products discussed are not intended to diagnose, treat, cure, or prevent any disease, and medical treatments require professional oversight.
Trust and Transparency: I only recommend products I trust. Most are items I use personally, while others are shared based on my professional trust in the clinical standards of partners like Ellie MD. Some links are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate I earn from qualifying purchases.
Have you ever felt like you’re fighting a battle with your own body that no one else understands?
Maybe for you, it was a diagnosis that seemed to come out of nowhere and changed everything. Maybe it was a long and frustrating cycle of dieting that always left you feeling worse than before. Or maybe it was a season of life—grief, stress, change—that took its toll, emotionally and physically, and you haven’t truly felt like yourself since.
If you’ve ever felt that way, I want you to know I see you. Because for me, it was all of the above. So many of you have seen my journey, but I wanted to share the real story behind it.
My Story Started Long Before the Scale
My relationship with my body was complicated from the start. Growing up, I was a product of 90s starvation diet culture, where being “skinny” was the goal, no matter how unhealthy the methods were.
In my early 20s, I was diagnosed with PCOS, and we began a long and painful journey to start our family. That journey included nine pregnancies. It’s still hard to type that number. Over several years, we experienced the heartbreak of three infant losses and six miscarriages. My body went through an absolute warzone of hormones, grief, emotional eating, and medical interventions like magnesium drips that caused insane fluid retention.
10 years ago at 30 weeks pregnant – yes THIRTY – we don’t make small babies
My Metabolism Had Officially Quit
By the time that chapter of our lives closed, my body felt completely foreign. It felt broken. My metabolism, for all intents and purposes, was non-existent. The old “calories in, calories out” formula was a joke. I once gained 20 pounds in three months from having one soda a month, with absolutely no other changes to my diet. It felt like I was being punished by my own body, and I was starting to believe I’d never have control again.
Finding Hope in Science
The turning point for me was realizing I didn’t need another diet; I needed a different set of tools. I started researching and learning about how my hormones and metabolic system were truly functioning (or not functioning). This is what led me to GLP-1 medications and peptides, like the ones I now get from Ellie MD.
For the first time, it felt like I wasn’t fighting my body anymore. Instead, I was giving it the support it needed to finally work with me. This was the useful, science-backed information I needed to finally find hope again.
This Isn’t Diet Culture – It’s Health
For the first time in my adult life, I have reached a healthy weight, and I’ve done it the HEALTHY way. There is no starvation here. In fact, I eat MORE now than I did before my journey began. The difference is that I’m making better choices, and my body is able to properly use the fuel I give it. This isn’t about fitting into a certain size; it’s about having the energy to live my life, feeling confident in my skin, and knowing I’m nourishing my body.
You’re Not Broken, and You’re Not Alone
I’m sharing all of this because I know how lonely that battle can feel. For years, I thought my body was broken beyond repair. If any part of my story sounds like your own, I just want you to know I see you, and you are not alone. Your story is valid.
Professional Disclosure: I provide BS-free metabolic education as a registered nurse and health coach for women navigating PCOS, perimenopause, and stubborn weight loss. While I share evidence-based research and nurse-informed support, please remember that I am not your nurse. The content shared here is for educational purposes only. It does not constitute medical advice, diagnosis, or treatment, and it does not establish a provider-patient relationship. Nothing on this site is a substitute for care from a licensed provider who knows your full health history. All opinions and content shared on this platform are my own and do not reflect the views or endorsements of my employer or the hospital where I am employed.
Scope of Practice and FDA: Per professional coaching guidelines, I may recommend over the counter (OTC) medications or supplements to support your wellness goals. However, I do not prescribe or recommend specific prescription medications. For prescription options, including GLP-1 tools, my role is to help you understand the available science so you can have an informed discussion with your licensed healthcare provider. These statements have not been evaluated by the Food and Drug Administration. Products discussed are not intended to diagnose, treat, cure, or prevent any disease, and medical treatments require professional oversight.
Trust and Transparency: I only recommend products I trust. Most are items I use personally, while others are shared based on my professional trust in the clinical standards of partners like Ellie MD. Some links are affiliate links or part of brand partnerships, which means I may earn a commission at no extra cost to you. As an Amazon Associate I earn from qualifying purchases.